Anterior Cervical Discectomy & Fusion (ACDF)
Removal of a herniated or degenerated cervical disc through a small incision at the front of the neck, followed by fusion of the adjacent vertebrae to restore stability and relieve nerve compression.
Radiculopathy
Myelopathy
Disc Herniation
Stenosis
When Is It Recommended?
ACDF is indicated when cervical radiculopathy, myelopathy, or disc herniation fails to respond to conservative care (physical therapy, medications, injections) — or when neurological deficits are progressing. Common conditions include pinched nerve roots, spinal cord compression, and cervical instability from trauma.
What to Expect
Surgery takes 1–2 hours per level. Most patients go home the same day or after one night. Full recovery typically takes 4–6 weeks. A cervical collar is worn for 4–6 weeks while fusion occurs. 90–95% of patients experience significant relief of arm pain and neurological symptoms.
Imaging
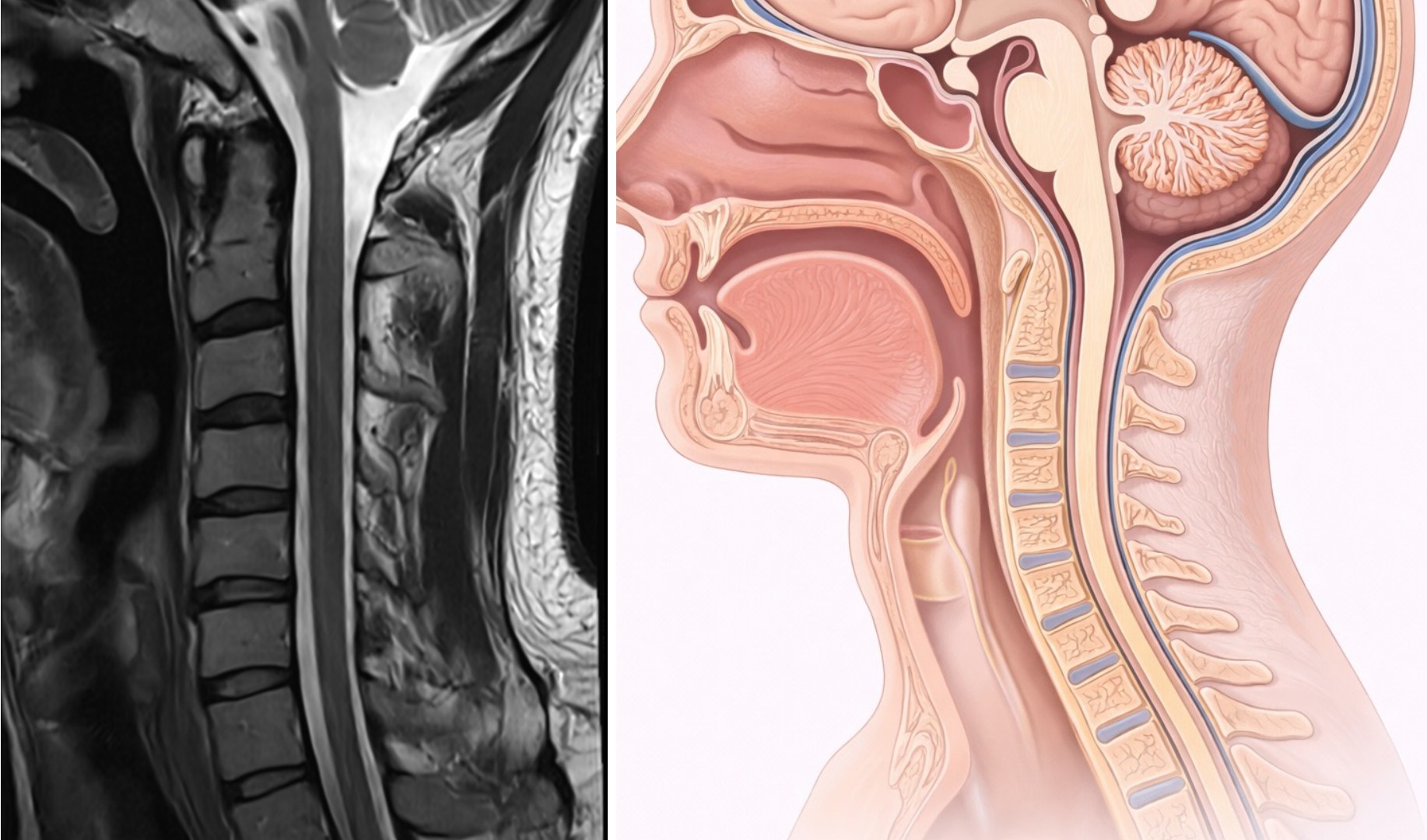
Normal Cervical Spine
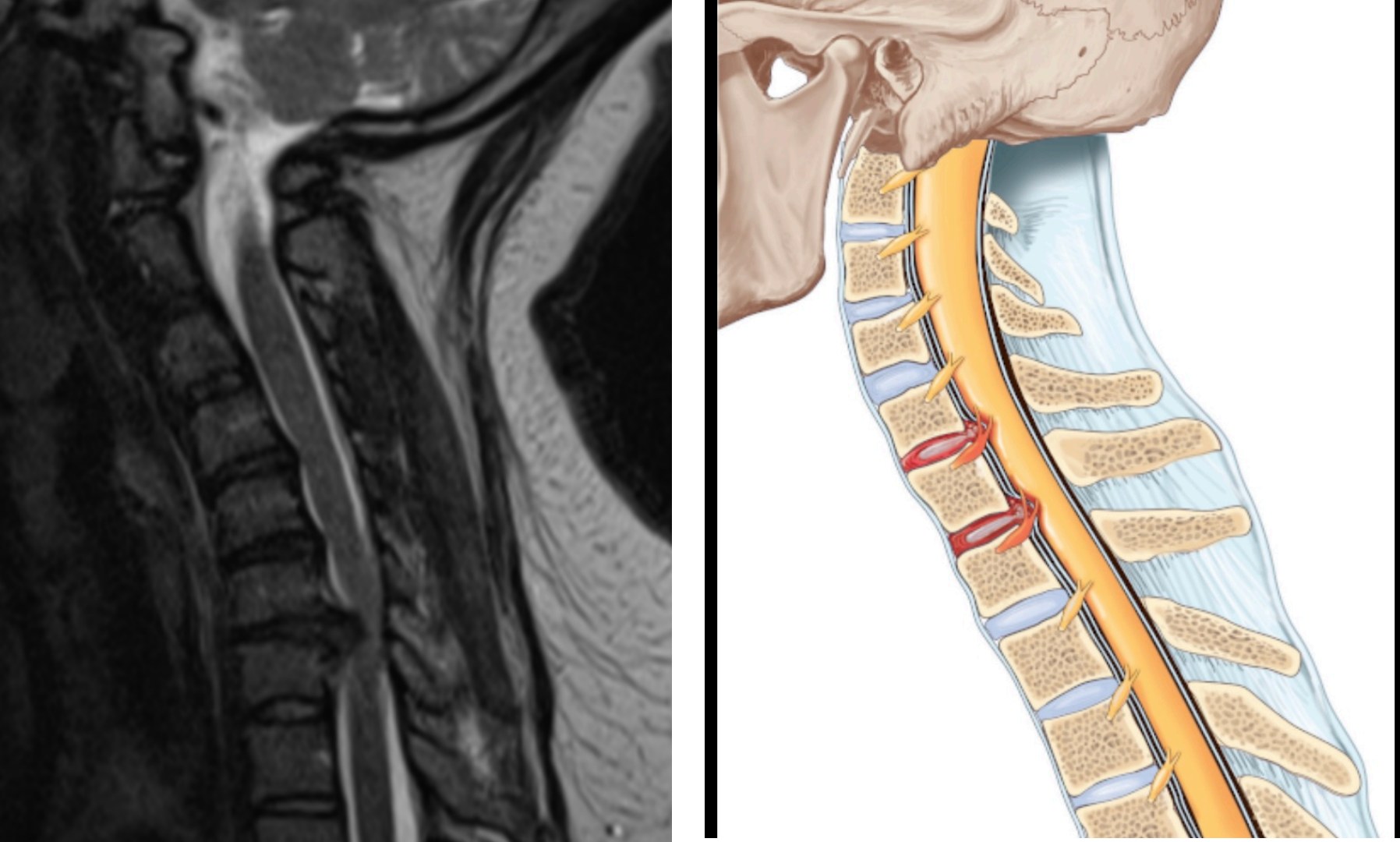
Cervical Disc Herniation
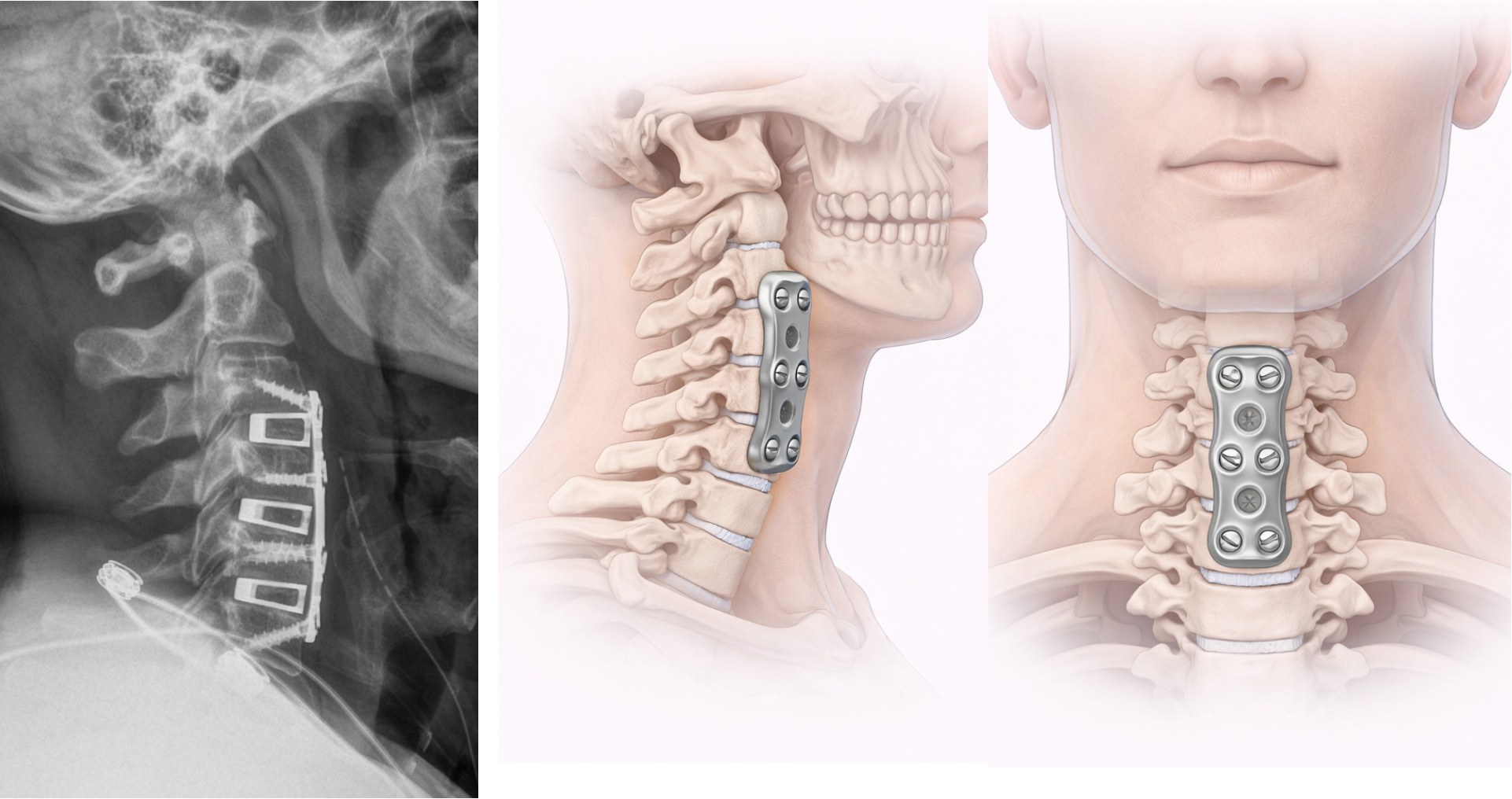
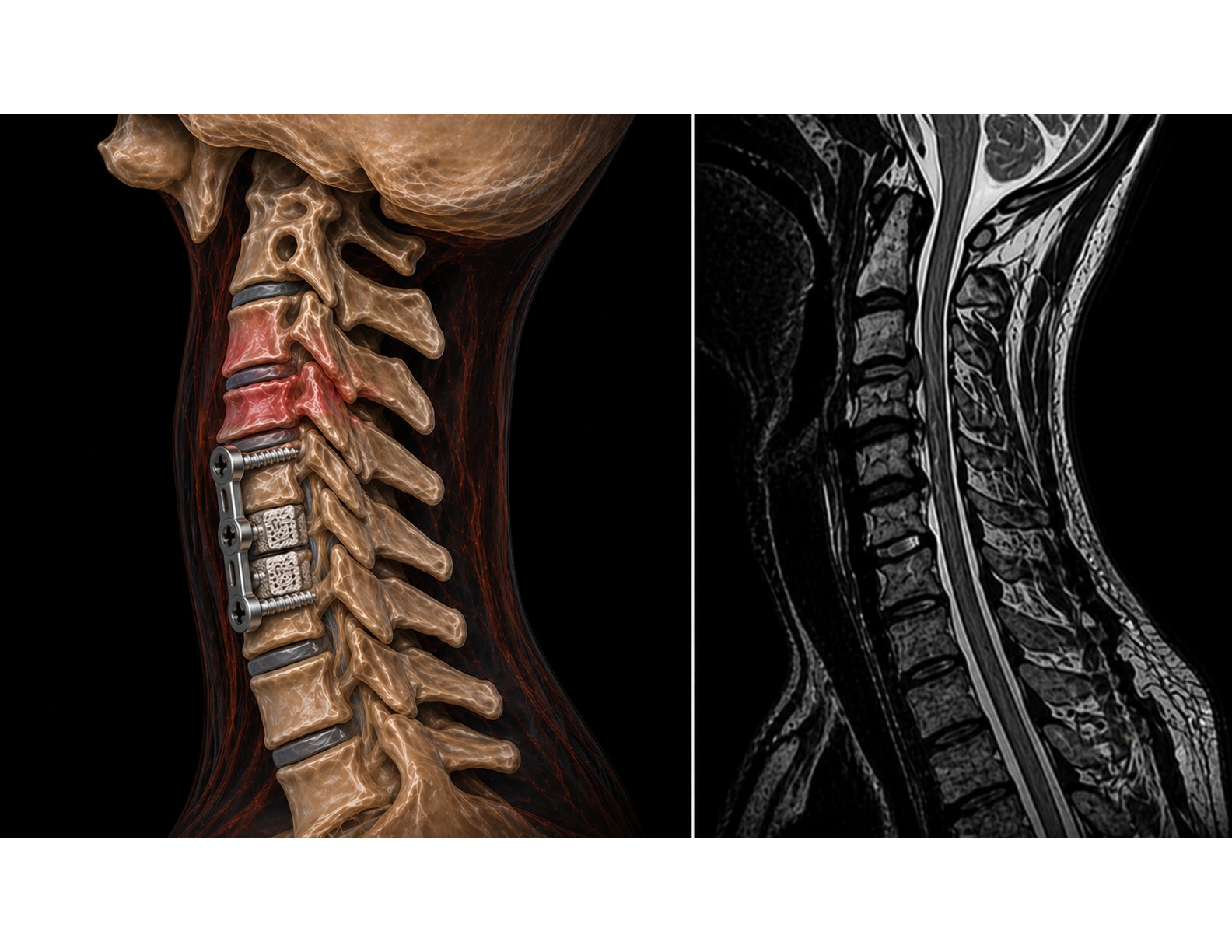
Post-Operative ACDF
Cervical Laminectomy & Fusion
Posterior decompression of the spinal cord by removing the lamina across multiple cervical levels, combined with instrumented fusion for stability — the definitive treatment for severe cervical myelopathy.
Myelopathy
Spondylotic Cord Compression
Ossified Ligament
Cervical Stenosis
Who Needs This Procedure?
Cervical myelopathy — compression of the spinal cord itself — causes hand clumsiness, leg weakness, balance problems, and in severe cases, bowel or bladder dysfunction. Unlike radiculopathy (pinched nerve), myelopathy rarely improves on its own and can become permanently disabling without surgery.
What to Expect
The lamina (bony roof) is removed to create space for the spinal cord, and the vertebrae are fused with rods and screws to prevent instability. Patients typically walk the first day post-op; hospital stay is 2–3 nights. A cervical collar is worn for 6–12 weeks. Most patients experience arrest of progression and meaningful functional recovery.
Imaging
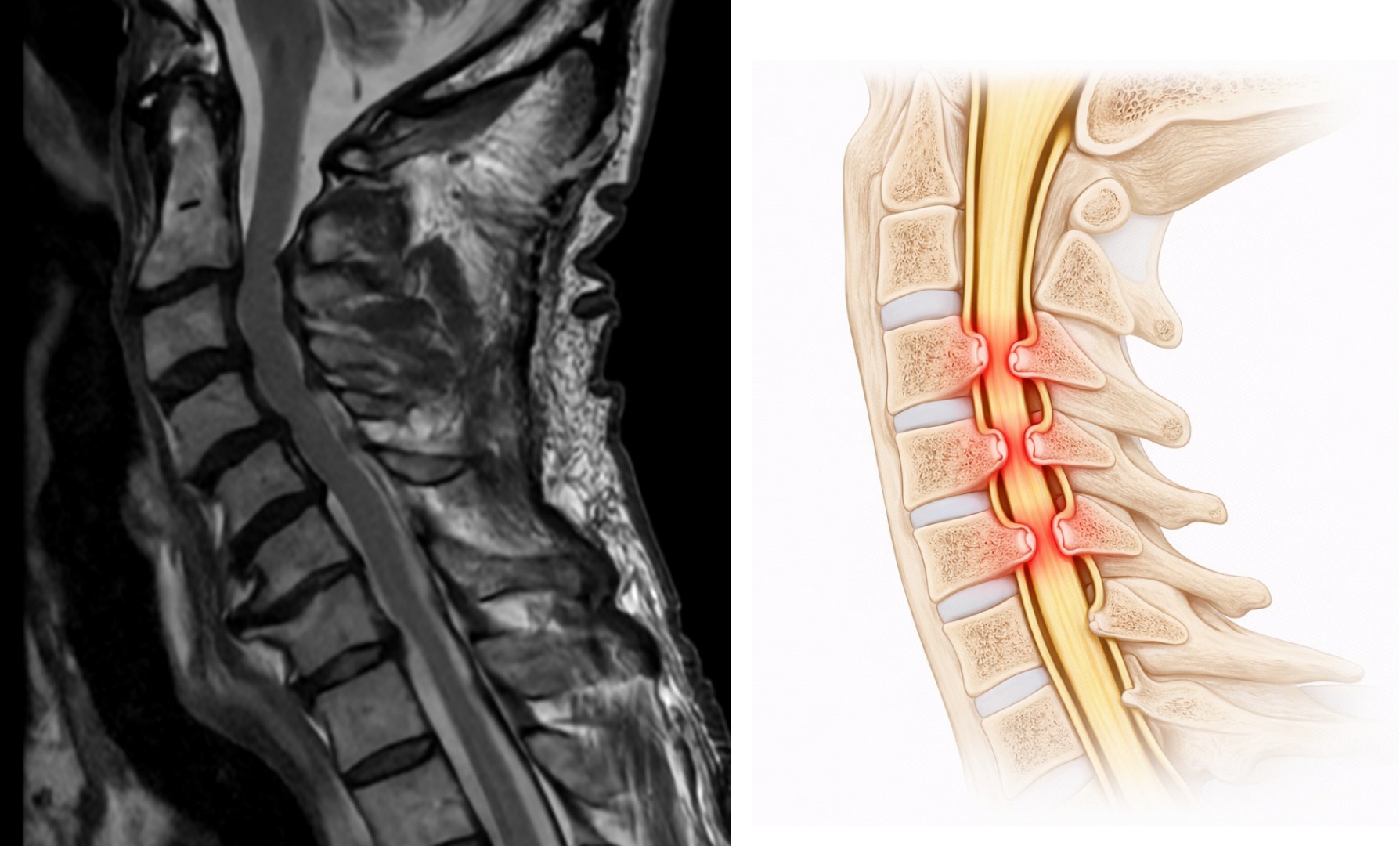
Cervical Stenosis
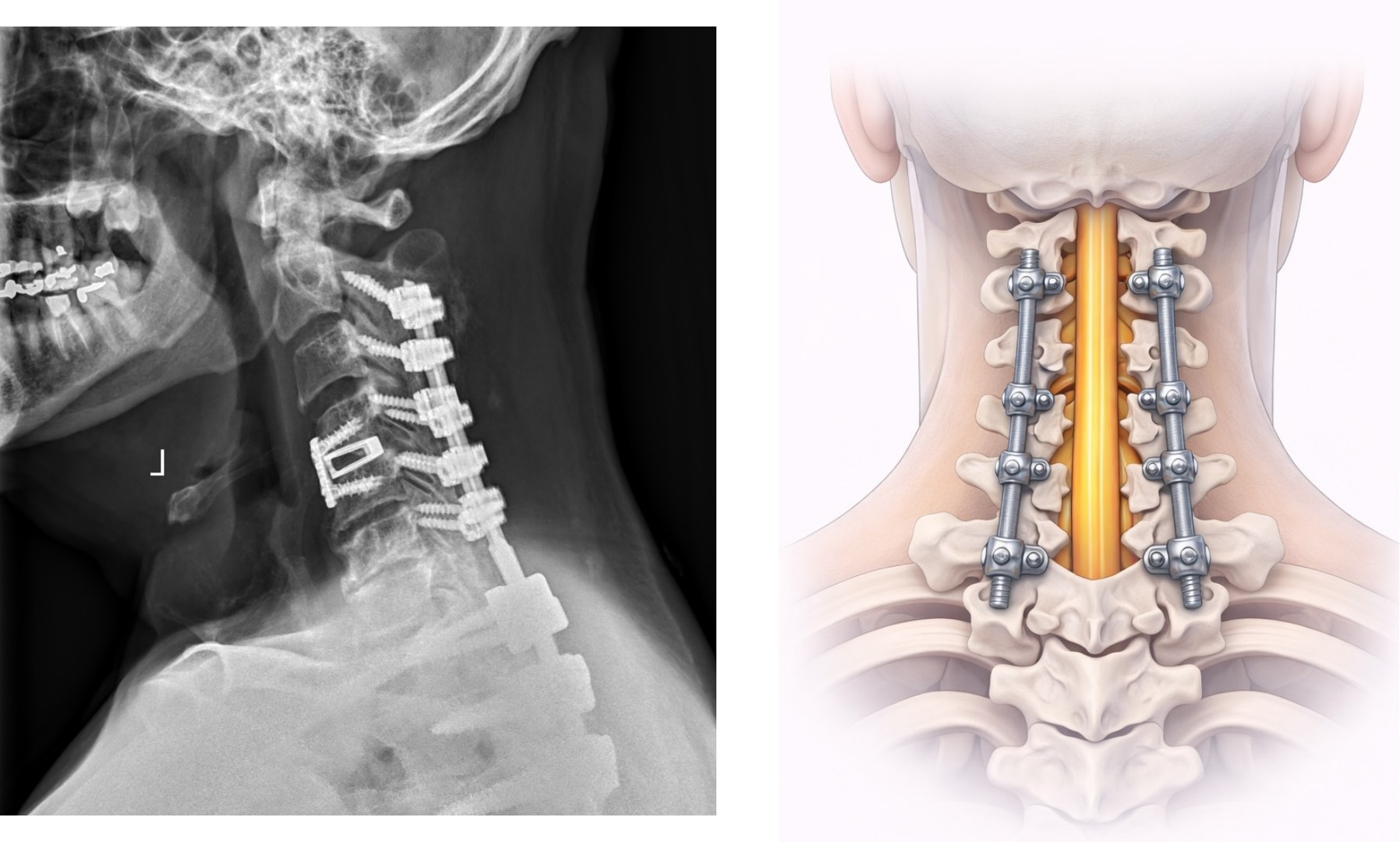
Post-Operative Fusion
Posterior Cervical Laminoplasty
A motion-preserving alternative to laminectomy — the lamina is reshaped and hinged open to expand the spinal canal without removing it, ideal for multilevel cervical myelopathy in patients with preserved cervical lordosis.
Myelopathy
Multilevel Stenosis
Ossified Ligament
Motion Preserving
Laminoplasty vs. Laminectomy
Rather than removing the lamina entirely, laminoplasty creates a hinge on one side and opens the lamina like a door, securing it in the open position with a small plate. This expands the spinal canal while preserving the posterior bony architecture — reducing the risk of postoperative instability and maintaining more natural neck motion.
What to Expect
Surgery takes 2–3 hours. Hospital stay is typically 2 nights. A soft cervical collar is worn for 4–6 weeks. Patients typically walk the first day post-op. Neck stiffness is expected and improves with physical therapy. Most patients see symptom stabilization or improvement within 3–6 months.
Imaging
Pre-Op: Stenosis
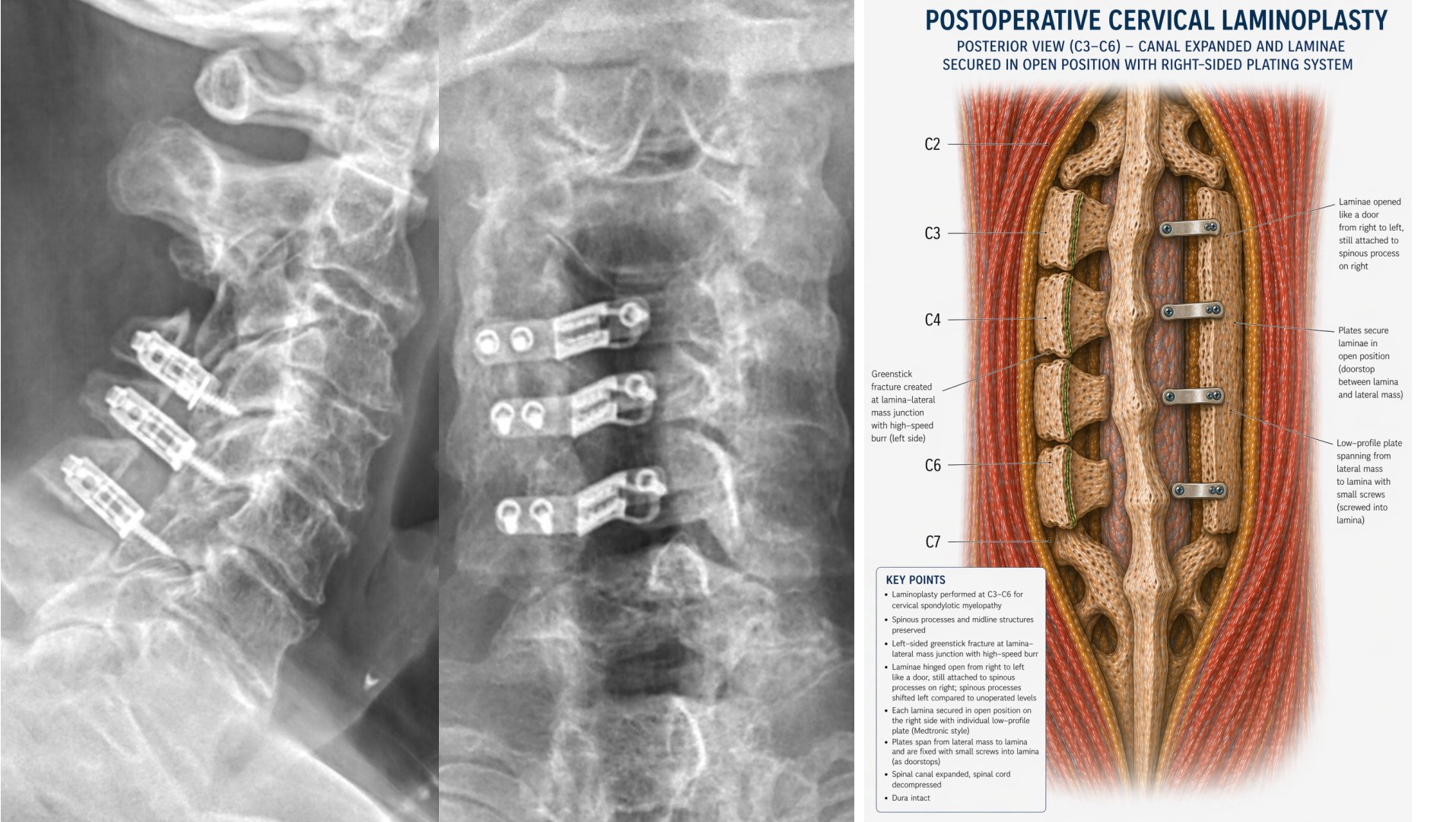
Post-Op: Laminoplasty
★ Area of Specialization
Cervical Revision Surgery
Corrective surgery for patients whose prior cervical procedure did not achieve the intended outcome — including pseudoarthrosis after ACDF, adjacent segment disease, failed disc replacement, and iatrogenic cervical kyphosis.
Pseudoarthrosis
Hardware Failure
Adjacent Segment Disease
Kyphosis Correction
Why Prior Surgery May Fail
The four most important causes of failure after cervical surgery are: pseudoarthrosis (failure of bone fusion), iatrogenic cervical kyphosis, failed disc replacement, and adjacent segment disease. Each has a distinct mechanism and requires a targeted surgical solution. Dr. Caridi has specialized expertise in the diagnosis and correction of all four.
Dr. Caridi's Approach
Revision cases require comprehensive review of prior operative reports, imaging, and implant records before a plan is formed. Dr. Caridi will explain clearly what went wrong previously and what corrective steps are proposed — so you can make a fully informed decision. Bring all prior surgical records and imaging to your consultation.
Imaging
Adjacent Segment Disease After Prior Cervical Fusion
Craniocervical Junction Surgery
Surgical management of pathologies at the skull-cervical junction — including Chiari malformation, atlantoaxial instability, rheumatoid pannus, and os odontoideum — one of the most anatomically demanding regions of the spine.
Chiari Malformation
Atlantoaxial Instability
Rheumatoid Pannus
Os Odontoideum
Why This Region Is Unique
The craniocervical junction houses the brainstem, upper cervical cord, vertebral arteries, and upper cranial nerves in a remarkably confined space. Pathology here — from Chiari malformation to atlantoaxial instability — can produce devastating consequences if unrecognized or untreated. The central surgical question is always: is decompression alone sufficient, or is fusion also required?
Chiari Malformation Decompression
Posterior fossa decompression relieves compression of the brainstem and spinal cord by removing bone at the back of the skull and expanding the dural covering. Surgery takes 2–3 hours; hospital stay is 2–4 nights. 85–95% of patients experience meaningful symptom relief.
Imaging
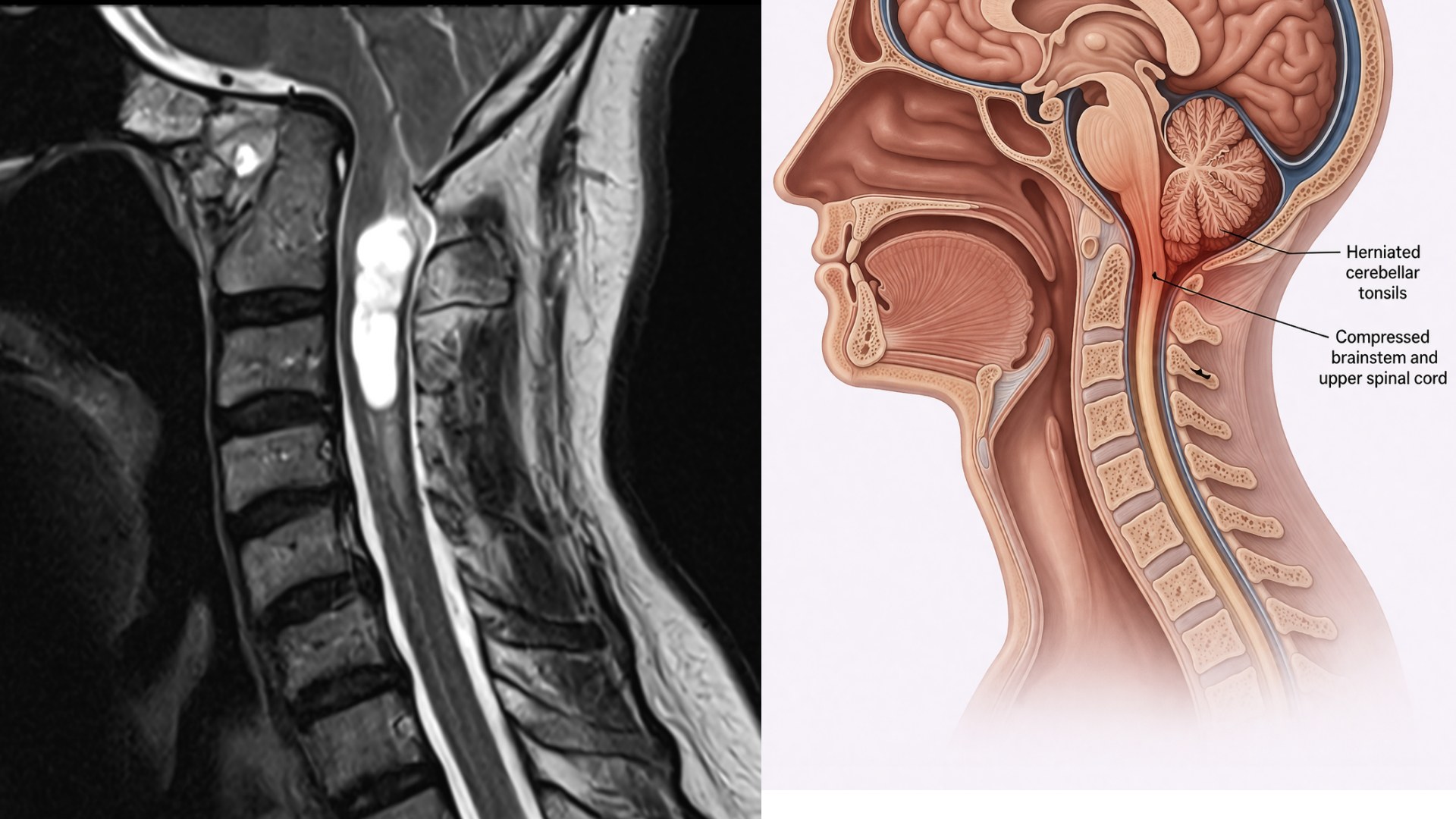
Chiari Malformation — MRI
Lumbar Microdiscectomy
Microsurgical removal of the herniated disc fragment pressing on a lumbar nerve root — the most common and highly successful spine surgery for sciatica and lower extremity radiculopathy, performed through a minimal incision.
Sciatica
Disc Herniation
Radiculopathy
Foot Drop
When Is It Recommended?
Surgery is typically considered after at least 6 weeks of conservative care (physical therapy, anti-inflammatories, epidural injections) has failed — or when progressive weakness, foot drop, or cauda equina syndrome is present. Most commonly affects L4–5 or L5–S1 levels.
What to Expect
Surgery takes about 1 hour through a 1-inch incision. Most patients go home the same day. Return to light activity in 1–2 weeks; full recovery in 4–6 weeks. Success rate for leg pain relief is approximately 90%. The disc can re-herniate in 5–10% of cases, which is why core strengthening rehabilitation is essential.
Imaging
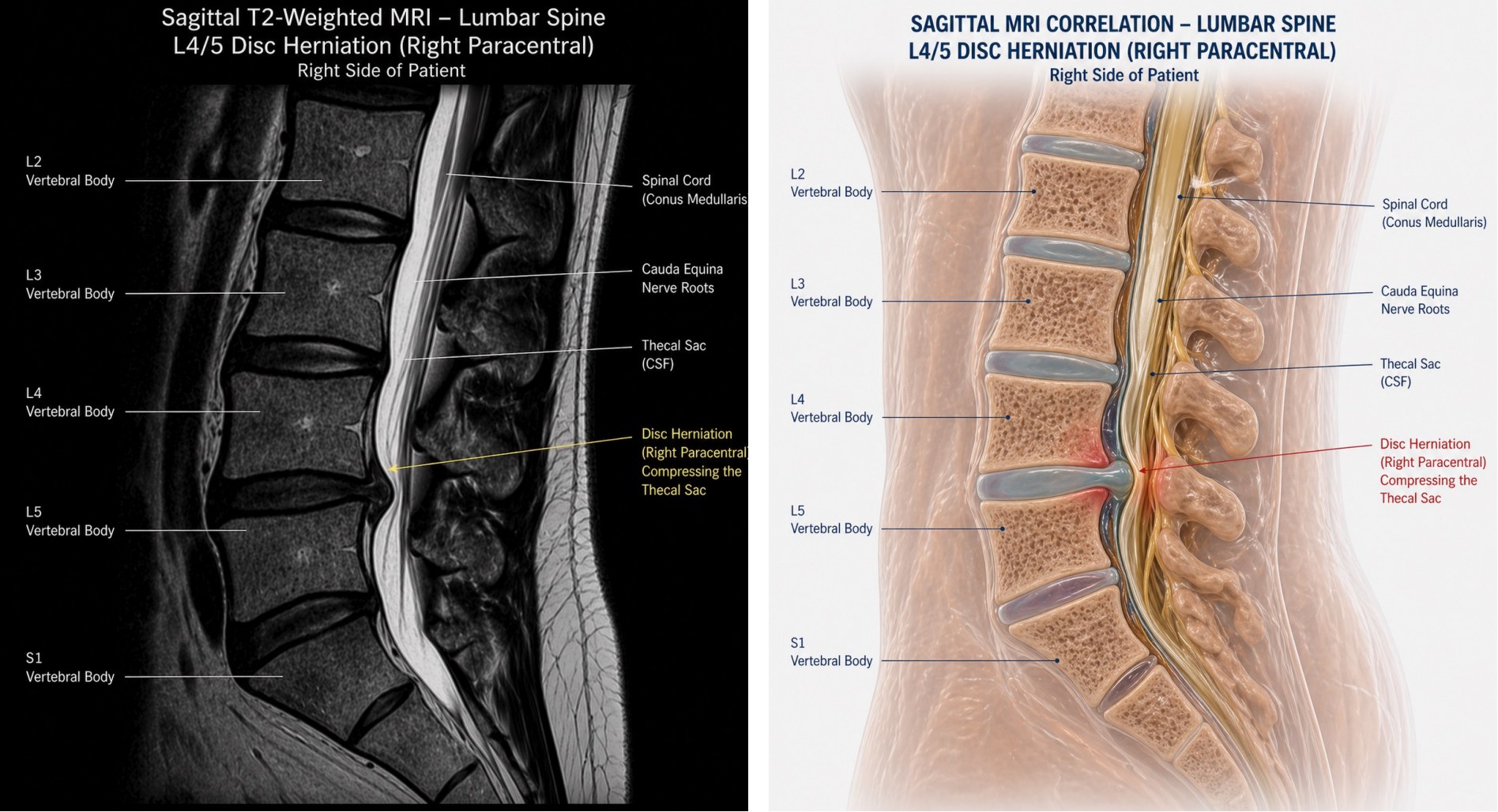
Disc Herniation — Sagittal
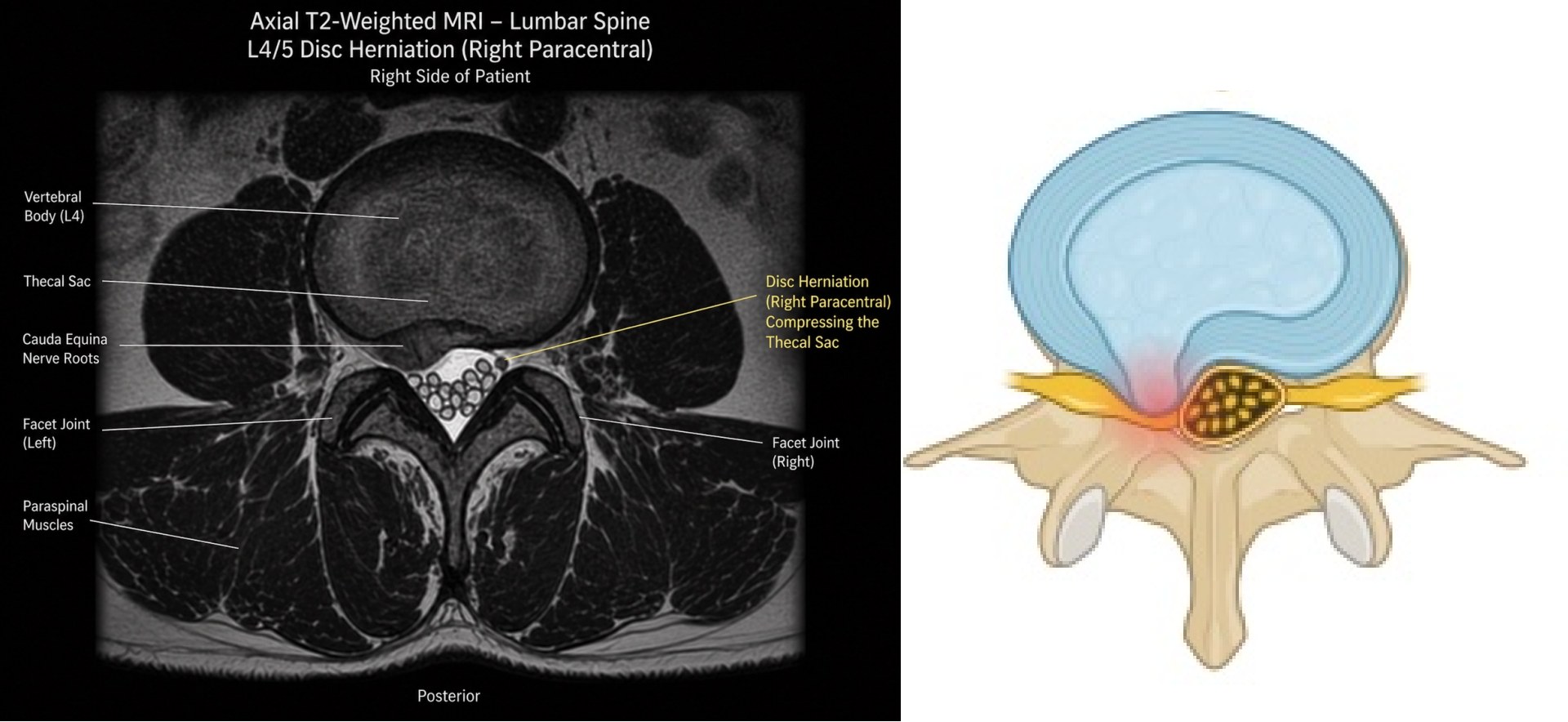
Disc Herniation — Axial
Lumbar Spinal Stenosis Surgery
Surgical decompression of the lumbar spinal canal to relieve nerve compression from bone spurs, thickened ligaments, and disc bulging — restoring the ability to walk and stand without pain.
Neurogenic Claudication
Spinal Canal Narrowing
Leg Pain & Weakness
Decompression
Understanding Lumbar Stenosis
Stenosis causes the spinal canal to narrow due to a combination of disc degeneration, bone spur formation, facet joint enlargement, and ligamentum flavum thickening. The signature symptom is neurogenic claudication — pain, cramping, or weakness in the legs when walking, relieved immediately by sitting or bending forward. Most commonly affects L4–5.
Surgical Decompression
A lumbar laminectomy removes the bone and thickened ligament compressing the nerves. When instability is present, fusion is added. Surgery takes 1–3 hours depending on levels involved. Most patients walk the same day. Return to normal activity in 4–8 weeks. Over 80% of patients achieve significant, durable relief of leg symptoms.
Imaging
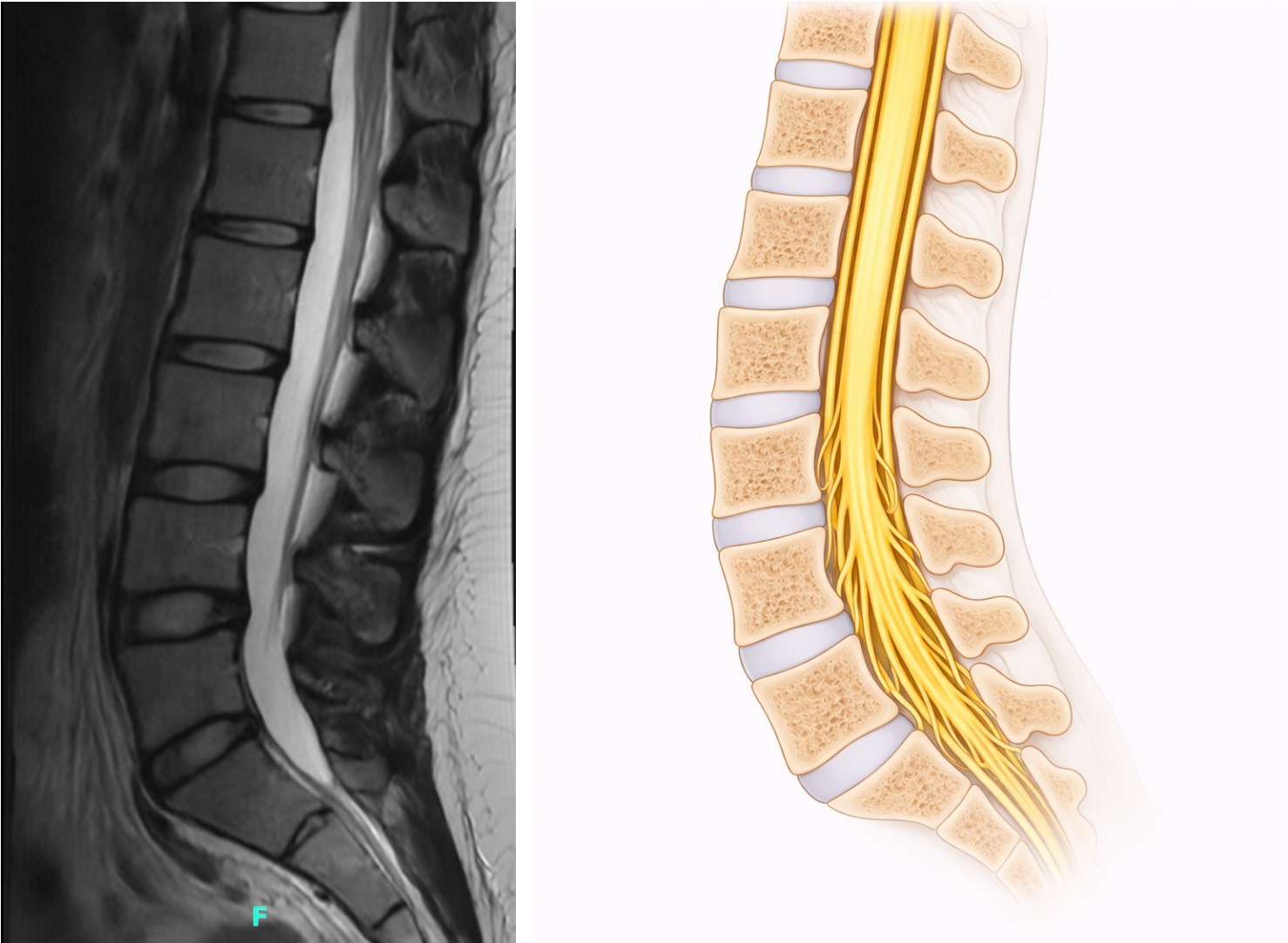
Normal Lumbar Spine
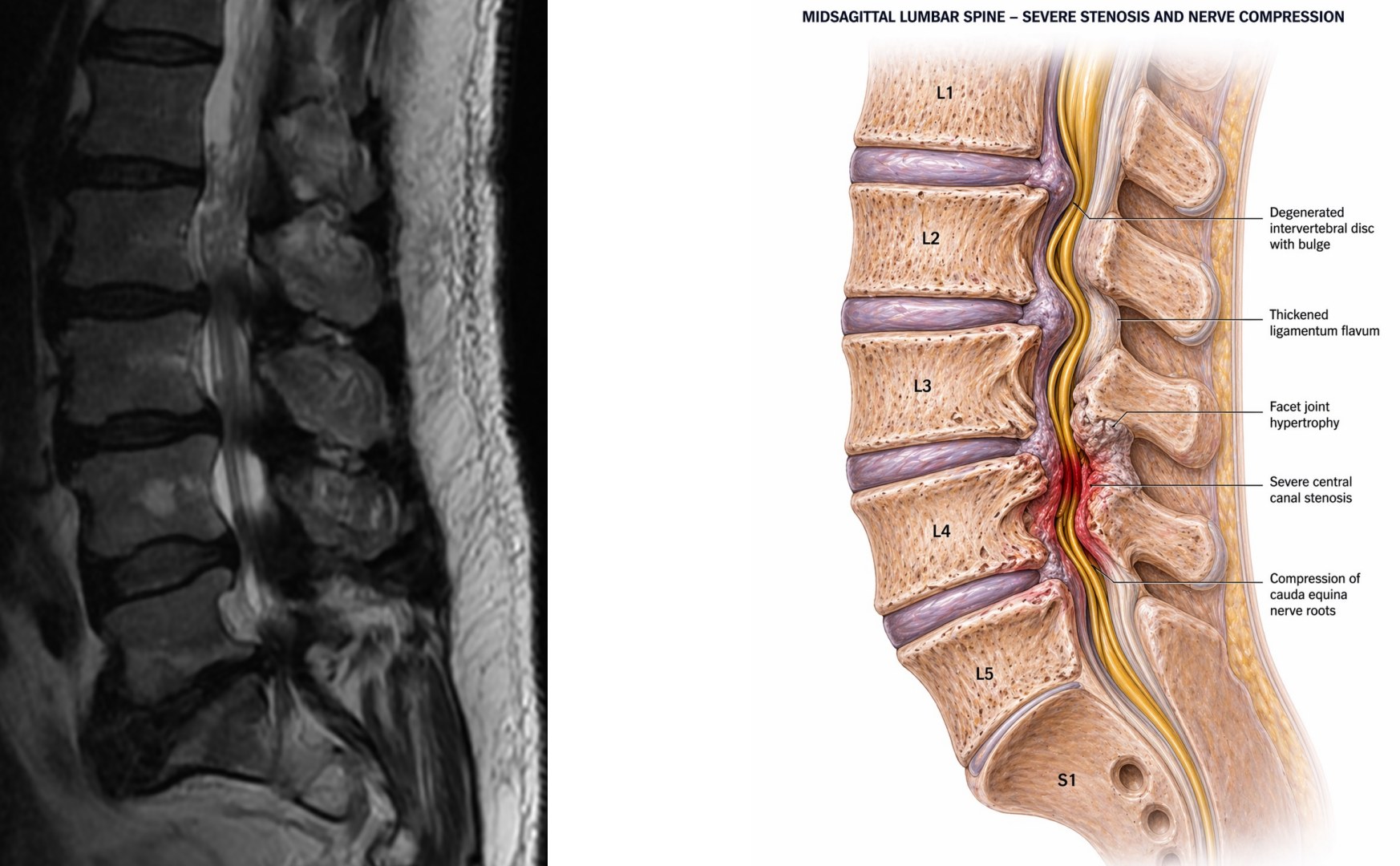
Lumbar Stenosis
Lumbar Spondylolisthesis Surgery
Surgical stabilization for vertebral slippage in the lumbar spine — decompressing the nerves compressed by the slip and fusing the unstable segment to prevent further progression and relieve back and leg pain.
Vertebral Slippage
Spinal Instability
Degenerative
Interbody Fusion
What Is Spondylolisthesis?
Spondylolisthesis occurs when one vertebra slips forward over the one below it, most commonly L4 on L5. The slip stretches and compresses nerves, causes stenosis, and destabilizes the disc and facet joints. Graded I–IV based on the percentage of slip; Grade I (0–25%) is most common and often managed conservatively. Grades II–IV typically require surgical consideration.
Surgical Treatment
Surgery involves decompressing the nerve roots and fusing the slipped vertebrae with a bone graft and pedicle screw instrumentation (using a posterior or transforaminal interbody fusion approach). Recovery involves 2–3 nights in hospital, a lumbar brace for 6–8 weeks, and physical therapy starting at 4–6 weeks. Over 85% of patients achieve significant relief of leg and back symptoms.
Imaging
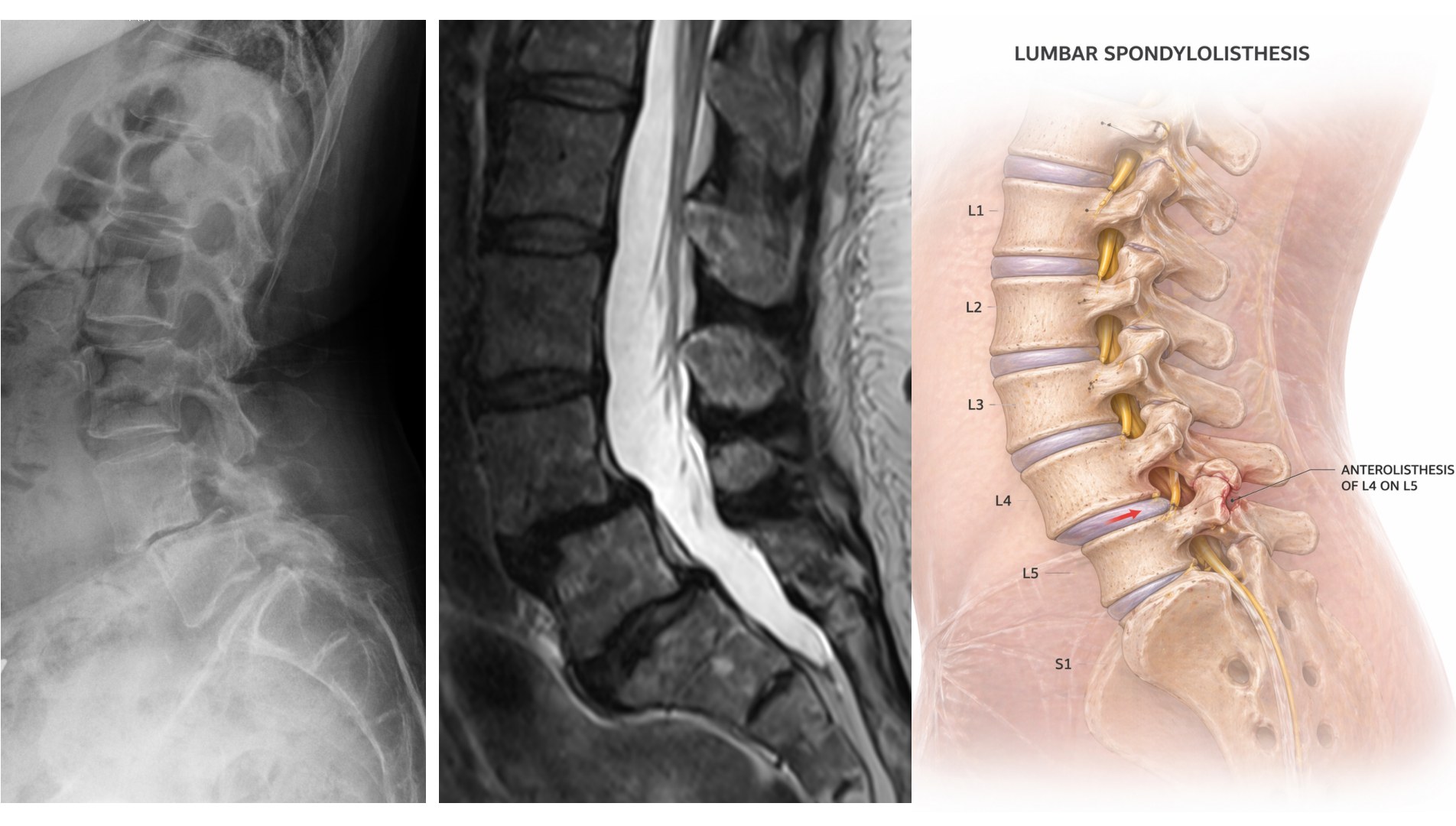
Lumbar Spondylolisthesis — L4 on L5
★ Area of Specialization
Lumbar Revision Fusion Surgery
Corrective surgery for lumbar fusion that has failed to heal, hardware that has loosened or broken, or new problems that have developed at adjacent spinal levels — requiring specialized expertise in complex reconstruction.
Pseudoarthrosis
Hardware Failure
Adjacent Segment Disease
Flatback
Why Lumbar Fusion May Fail
The three most common causes of failure are: pseudoarthrosis (the bone graft never healed, leaving a painful false joint), iatrogenic flatback deformity (excessive straightening of the lumbar curve causing forward lean and chronic pain), and adjacent segment disease (accelerated degeneration above or below the fusion). Each requires a distinct surgical correction.
Dr. Caridi's Approach
Revision surgery demands comprehensive review of prior records, imaging, and implant documentation before any plan is formed. Bring all prior surgical records to your consultation. Dr. Caridi will explain precisely what failed and what corrective approach is recommended.
Imaging
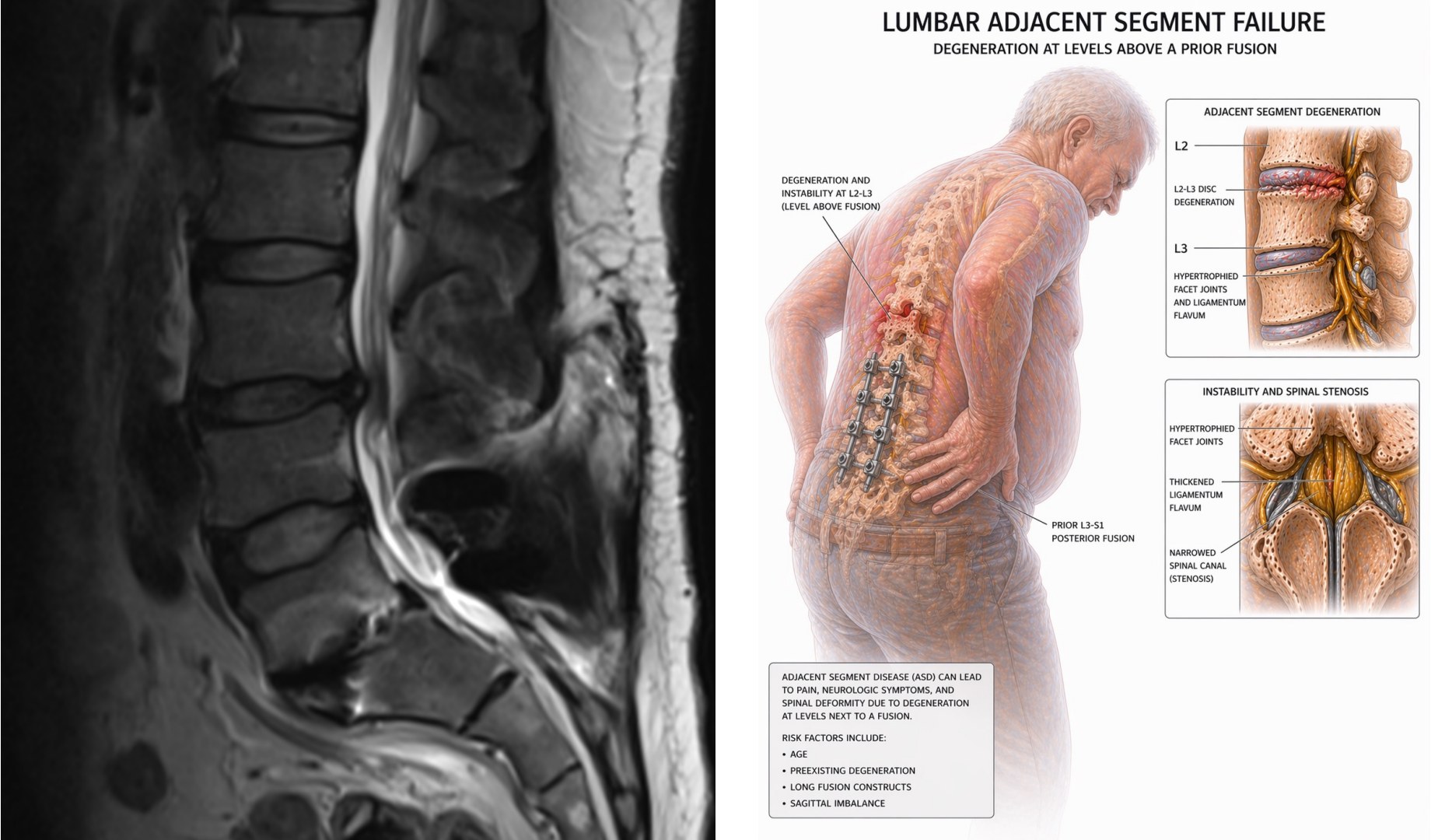
Adjacent Segment Disease After Prior Fusion
★ Area of Specialization
Flatback Deformity Correction
Surgical restoration of lumbar lordosis (the spine's normal inward curve) for patients with sagittal imbalance — correcting the forward-leaning posture that causes chronic pain, exhaustion, and loss of function.
Sagittal Imbalance
Lumbar Hypolordosis
Osteotomy
Deformity Correction
What Is Flatback Deformity?
The healthy lumbar spine has a gentle inward curve (lordosis) that keeps the body balanced over the hips and ankles. When this curve is lost — from degenerative disease, prior surgery, or aging — patients must compensate by bending their knees and thrusting their hips forward, a constant exhausting fight against gravity. The sagittal vertical axis (SVA) measures alignment; normal is less than 5 cm.
Surgical Correction
Correction involves osteotomies (controlled bone cuts) to recreate lordosis, combined with instrumented fusion to hold the corrected alignment. This is among the most complex procedures in spine surgery. Recovery spans several months with supervised physical therapy. Outcomes can be life-changing — patients stand upright and walk without exhaustion for the first time in years.
Imaging
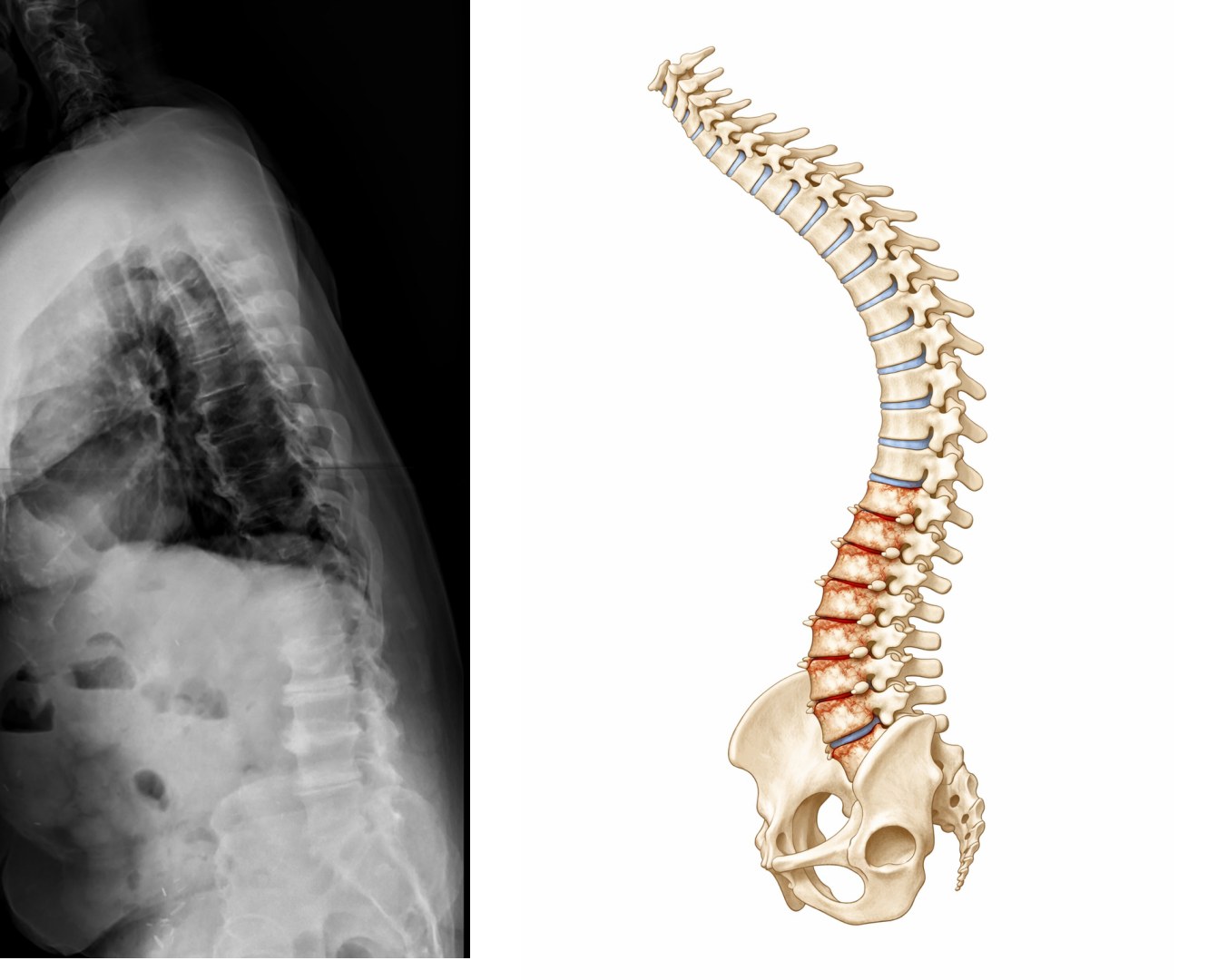
Flatback Deformity — Sagittal Imbalance
Intradural Spinal Tumor Resection
Microsurgical removal of tumors arising within the dural sac — including schwannomas, meningiomas, ependymomas, and astrocytomas — the majority of which are benign and curable with complete resection.
Schwannoma
Meningioma
Ependymoma
Intramedullary
Extramedullary vs. Intramedullary
The critical distinction is whether the tumor is outside the spinal cord (extramedullary — 65–70% of intradural tumors) or within the cord itself (intramedullary — 25–30%). Extramedullary tumors such as schwannomas and meningiomas are usually benign, displace the cord without invading it, and are highly curable with complete resection. Intramedullary tumors arise from cord tissue and are more surgically challenging.
Surgical Outcomes
Intradural spinal tumors are among the most surgically rewarding conditions to treat — complete resection often produces dramatic recovery of neurological function, particularly when treated before irreversible cord injury occurs. Intraoperative neurophysiologic monitoring (motor and sensory evoked potentials) is used throughout to protect neurological function.
Imaging
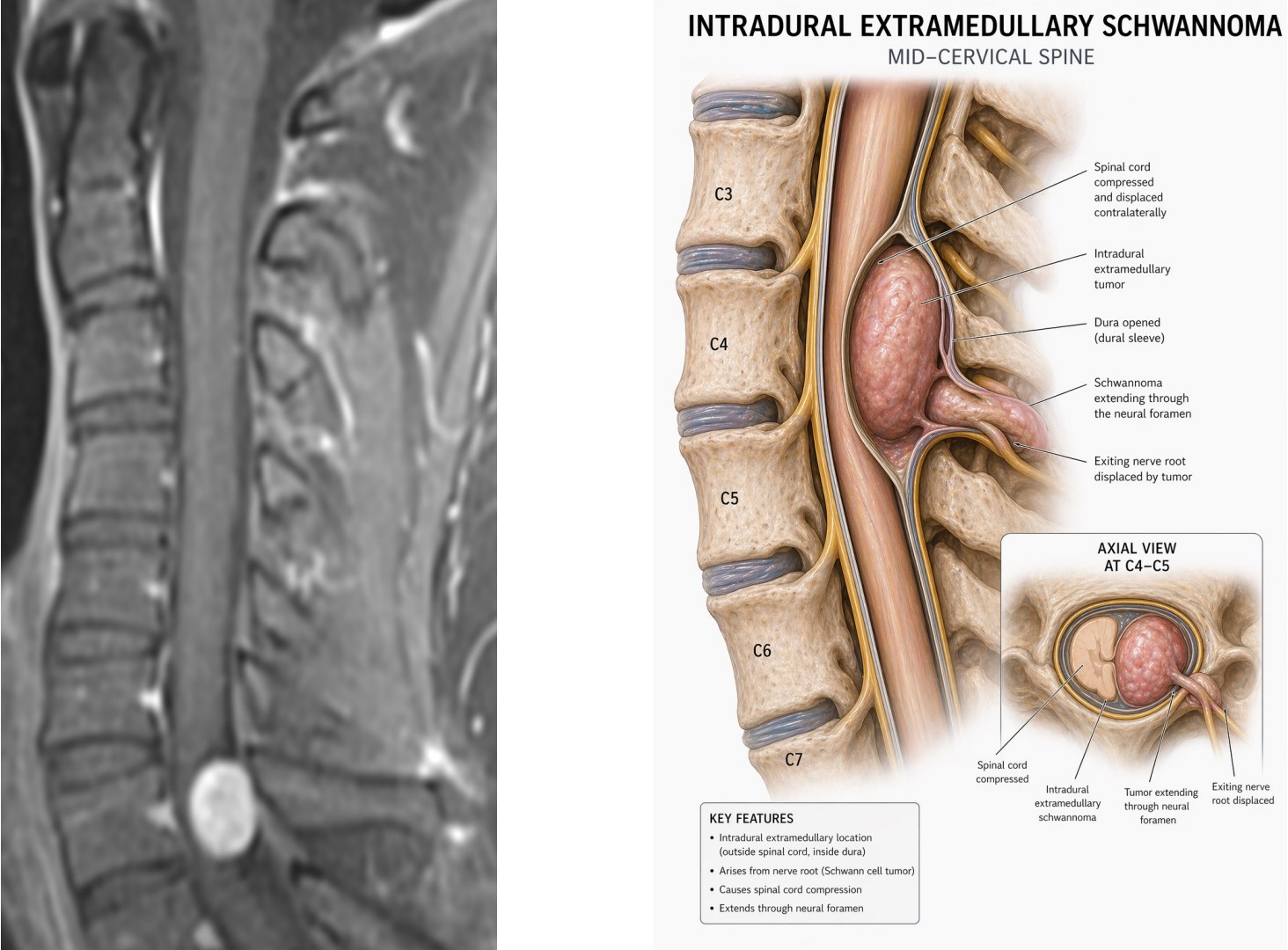
Intradural Spinal Tumor — MRI
Spine Health & Conservative Care
Comprehensive education on back pain prevention, spine-healthy body mechanics, and targeted exercise — most back pain can be prevented and managed without surgery through the right habits and care.
Back Pain
Body Mechanics
Exercise
Prevention
Dr. Caridi's Philosophy
Surgery is always the last resort. Back pain affects up to 80% of people at some point in their lives, yet the vast majority respond well to conservative care — physical therapy, targeted exercise, ergonomic adjustments, and medications. Dr. Caridi always exhausts non-surgical options before recommending an operation.
Conservative Care First
The spine health guide covers proper lifting mechanics, ergonomic workstation setup, sleeping positions, core strengthening exercises, and strategies for managing flare-ups. Download the free guide to learn how to protect your spine and reduce the risk of surgery.
